Roe v. Wade made abortion legal for all women in 1973. Even so, state legislators have been weaving a web of laws to incrementally restrict abortions ever since. This includes funding restrictions and, in recent years, the so-called TRAP laws that place excessive, expensive and unnecessary rules on clinics and abortion providers.
In Washington, Congress has undermined Roe v. Wade via the federal budget. After abortion first became legal, Medicaid, the joint federal-state program that provides basic health-care services to people with limited incomes, covered abortions just like other health care procedures. But three years later, Rep. Henry Hyde (R-IL) attached an amendment to a Department of Health and Human Services appropriations bill to ban the use of Medicaid funds to provide abortions.
Hyde knew this would put abortion out of reach for many low-income women. “I certainly would like to prevent, if I could legally, anybody having an abortion — a rich woman, a middle-class woman or a poor woman,” Hyde said at the time. “Unfortunately, the only vehicle available is the … Medicaid bill.” In the 1990s three very narrow exceptions were added to Medicaid coverage of abortion: if a woman’s life is at risk, or if her pregnancy is the result of rape or incest.
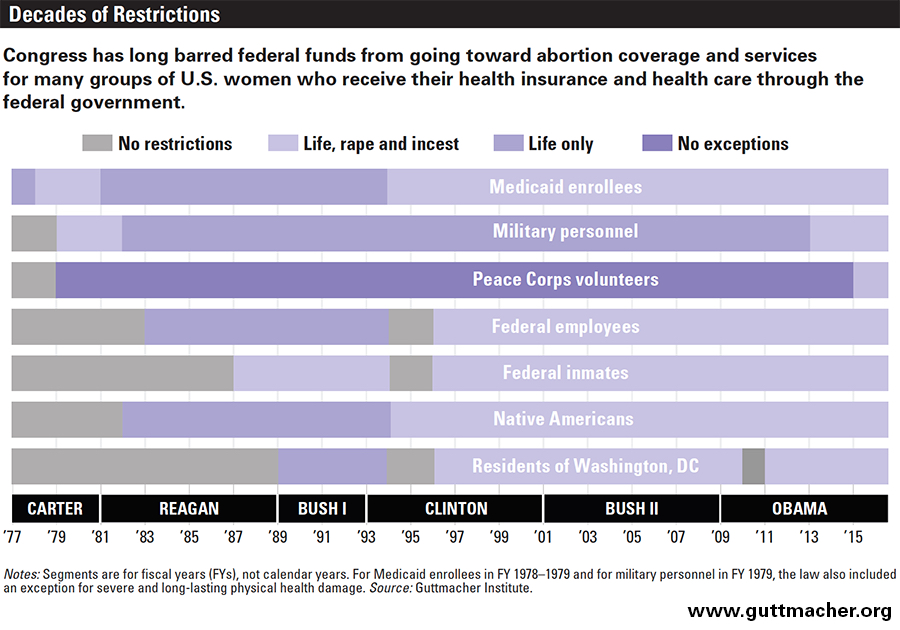
The Hyde Amendment impacts all federal programs that provide or pay for women’s reproductive health services, including federal prisons and ICE detention centers; the Peace Corps; Indian Health Services; the Federal Employees Health Benefits Program; and the US military’s TRICARE program. There is also language in the Affordable Care Act that restricts the abortion coverage in plans sold through the marketplace and for women who receive federal income-based subsidies to buy private health insurance.
Denied
When women are denied abortion coverage by federally funded health-insurance programs, they often don’t have the money to pay out-of-pocket. In-clinic surgical abortions can cost up to $1,500 in the first trimester, or $3,000 in the second trimester. The cost in a hospital is often more. The abortion pill, known as a medication abortion, can cost as much as $975. According to the Guttmacher Institute, the average cost of a first-trimester surgical abortion in 2011 was $480, and an early medication abortion was $504. Nearly 60 percent of the women who delayed their procedures said it was because they had to raise the money or search for a low-cost provider. Others divert money that they and their families need to live on. In addition to the expense of the procedure, there is the cost of travel and missing work. One in four women is forced to carry her unwanted pregnancy to term.
Medicaid
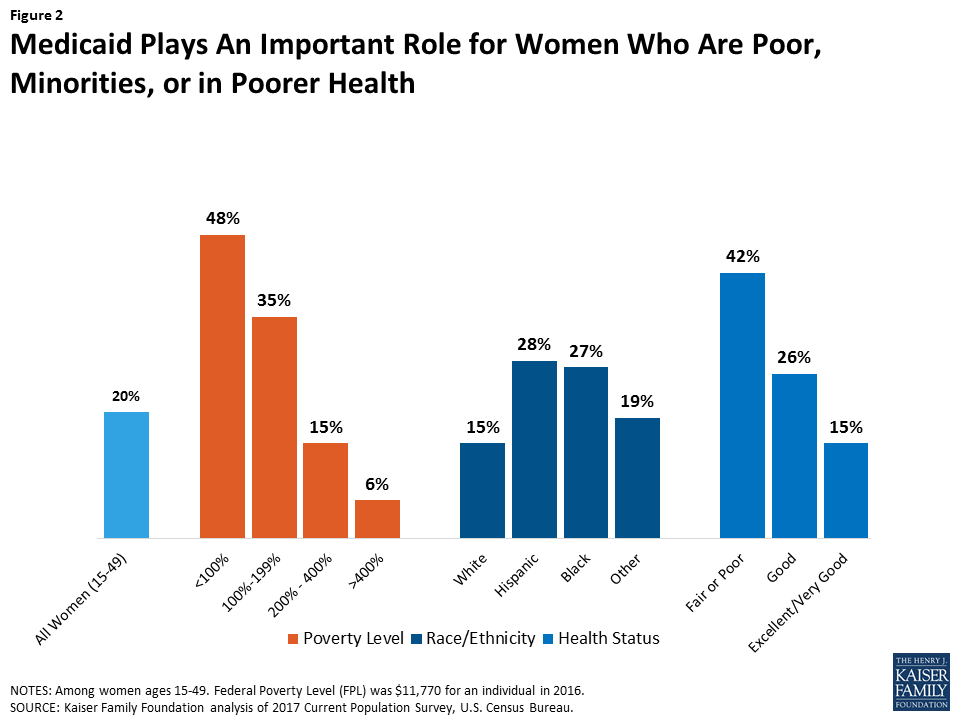
The Hyde Amendment added a temporary “rider” to the Medicaid funding bill that is approved by Congress every year. And every year low-income women are disproportionately denied coverage to end unwanted pregnancies, except in extreme cases. Medicaid is the largest source of health-care funding for low-income and poor people in the United States. One in five of all women of reproductive age depend on Medicaid’s sexual and reproductive health services. In 2015, 31 percent of this group was black, 27 percent was Hispanic and 16 percent were white.
State Funding
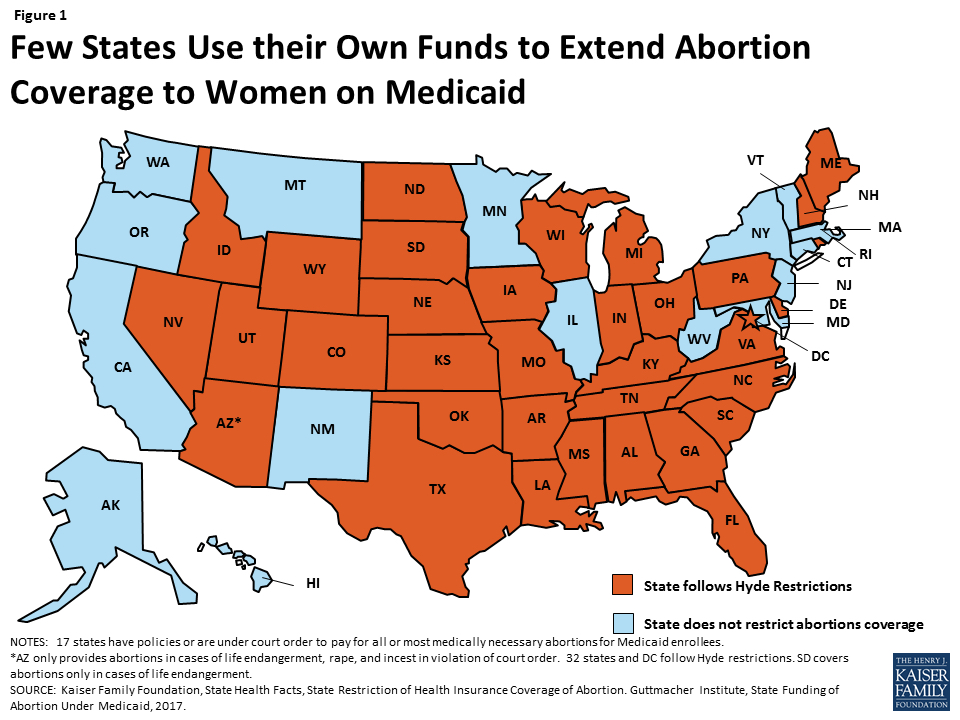
While the Hyde Amendment bars Medicaid from using federal funds to cover abortion, states may use their own nonfederal funds to cover the cost. Seventeen states have a policy requiring the state to provide abortion coverage under Medicaid, but according to the Guttmacher Institute, just 15 states appear to be doing so in practice. In September 2017, Illinois became the first state in decades to enact a law that expanded Medicaid and state employee insurance to cover abortion.
TRICARE
Sixteen percent of the US military — more than 355,000 individuals — are women, most of whom are in their childbearing years. According to a military study last year, the rate of unwanted pregnancy in the armed services ranges from 50 to 62 percent, the same as in the civilian population.
TRICARE, the military health-care program for service members, reservists and dependents, is supposed to cover birth-control pills and other forms of contraception, but access can be challenging. A study conducted in 2013 found that, among the women they surveyed, one-third could not get the birth control they wanted before deploying, and 41 percent had trouble refilling prescriptions while on duty. Getting pregnant is taboo “in theater,” when a woman is actively deployed, and it can derail her career. Even so, Congress made the ban on funding abortion services for servicewomen and their dependents permanent in 1984, except for life endangerment. An amendment introduced by Sen. Jeanne Shaheen (D-NH) in 2012 extended the coverage to cases of rape or incest. In all cases, the Department of Defense bans military treatment facilities from performing abortions, even if the patient pays out of pocket.
Indian Health Service
Some 2 million Native Americans get their health care from the Indian Health Service (IHS), which is funded through the Department of Health and Human Services. The IHS is often the only option on a remote reservation, but the federal government will allow abortion coverage only if a woman’s life is at risk or in cases of rape and incest. Even then, according to a 2014 report, 85 percent of the IHS Service Units the researchers contacted were out of compliance with the IHS abortion policy. Many IHS clinics do not have abortion facilities at all. For rural Native women the trip to a city to terminate a pregnancy can be prohibitively expensive, requiring transportation, often a waiting period, and overnight lodging.
Peace Corps
There are some 7,200 US citizens who volunteer for the Peace Corps. Of them, 63 percent are women. But until recently the federal government has prohibited coverage, with no exception, for abortion services requested by volunteers or trainees — many of whom live on a monthly stipend of $250 to $400. In 2015, coverage was expanded to include cases of rape, incest or life endangerment. If a volunteer decides to pay out-of-pocket for an abortion, however, there are no restrictions on funding a medical evacuation to a location where abortions are legal and there are adequate medical facilities.
Financial Help
For women struggling with the financial burden of an abortion procedure, there are organizations that offer help.
Although Medicaid covers abortion procedures in certain states, for most, that is only the case when a woman seeking an abortion became pregnant as a result of rape or incest, or is in a life-threatening health condition as a result of her pregnancy.
Clinics offer some financial assistance and there are local organizations in many states that offer help. The National Network of Abortion Funds helps women cover the cost of an abortion in 38 states. Some of the financial help NNAF provides is for the costs associated with an abortion beyond the procedure itself, such as travel, child care, lost work hours, feminine pads and pain medication for the recovery period.